Grand Rounds
Practical Strategies for Management of Lenalidomide-Associated Cytopenias in Myelodysplastic Syndromes With del(5q)
Sandra E. Kurtin,(1) PhDc, ANP-C, AOCN®, Jean A. Ridgeway,(2) DNP, NP-C, AOCN®, and Sara Tinsley,(3) PhD, ARNP, AOCN®
1)University of Arizona and Arizona Cancer Center, Tucson, Arizona; 2)University of Chicago Medical Center, Chicago, Illinois; 3)H. Lee Moffitt Cancer Center and Research Institute, Tampa, Florida
Authors’ disclosures of potential conflicts of interest are found at the end of this article.
J Adv Pract Oncol 2017;8:721–728 |
https://doi.org/10.6004/jadpro.2017.8.7.5 |
© 2017 Harborside™
 ABSTRACT
ABSTRACT
Case Study
A male patient aged 67 years with a 2-year history of refractory anemia and myelodysplastic syndromes (MDS) with del(5q) started lenalidomide (Revlimid) treatment as a participant in the MDS-001 trial (List et al., 2005). At the time of the study, this patient had been transfusion-dependent since 2001, and at study entry he had received a total of 12 units of red blood cells (RBCs). The patient started lenalidomide at 25 mg daily for 21 days of each 28-day cycle on April 2, 2002. (Please note that as a result of subsequent trials, the approved starting dose for lenalidomide in patients with del[5q] MDS is 10 mg.) The patient developed treatment-related pancytopenia in the first 3 weeks of treatment (see Figure on next page).
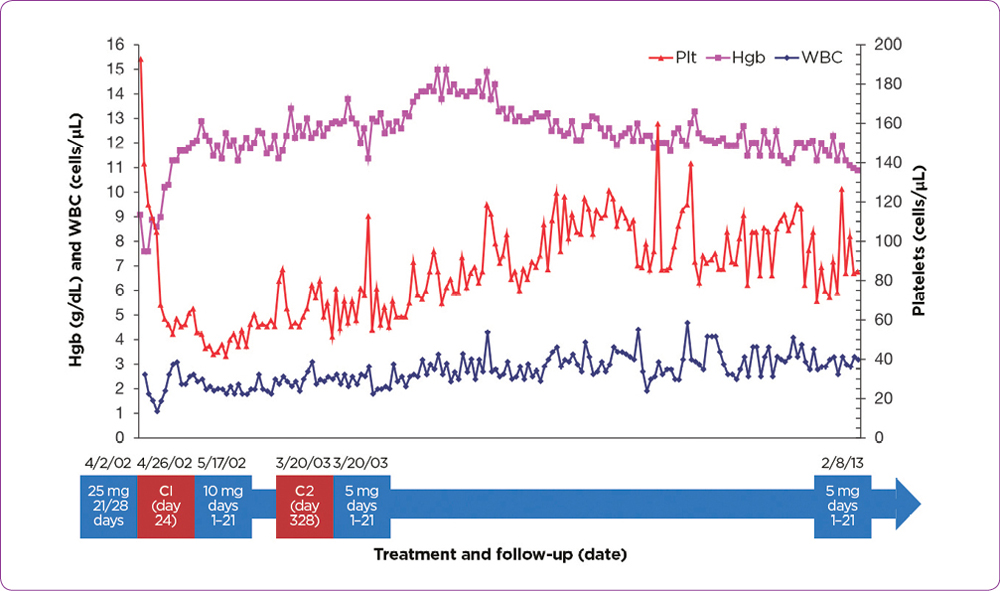
On day 24, lenalidomide was withheld. Platelet and white blood cell (WBC) counts were recovered during a 21-day period, and treatment was resumed with lenalidomide at 10 mg daily. During this initial dose interruption, the patient’s hemoglobin level improved. He achieved RBC-transfusion independence (TI) during week 5 of treatment—his last RBC transfusion was on April 22, 2002.
Bone marrow (BM) analysis, including fluorescence in situ hybridization, after 3 months of therapy, did not show the del(5q) abnormality. A repeat BM analysis after 57 months of treatment revealed minimal residual dyspoiesis, normal metaphase cytogenetics, and normal cell morphology. Subsequent BM biopsies showed transient trisomy 8 abnormalities but no del(5q) abnormality. The patient required one additional dose reduction during the first year of treatment. The patient did not require hospitalization during lenalidomide treatment but did have a history of seasonal allergies and a propensity for acute sinusitis. He received a single dose of pegfilgrastim (Neulasta) and a short course of antibiotics for active infections, generally one course of antibiotics per year.
This patient continued on lenalidomide at 5 mg daily for 21 days of every 28-day cycle without further dose reduction. The patient achieved durable RBC-TI and continued to receive treatment for more than 11 years. The levels of hemoglobin, platelets, and WBCs for an 11-year period in this patient are shown in the Figure. This patient had one normal platelet count in 11 years of lenalidomide treatment but no bleeding episodes. The average platelet count in the 11-year period was 67 × 1,000/∝L (normal range, 150–425 × 1,000/∝L). Similarly, the WBC count remained below normal, with an average of 3.1 × 1,000/∝L (normal range, 3.4–10.4 × 1,000/∝L). He remained active and continued working as an aerospace engineer until age 75.
This case demonstrates how effective management of cytopenias, through dose interruptions and modifications in the early weeks of treatment, helps to enable long-term lenalidomide treatment and a high quality of life. Despite the persistence of moderate, asymptomatic cytopenias, the patient was able to remain on lenalidomide therapy and maintained RBC-TI for more than 11 years. The patient died on October 4, 2014, at age 79.5, due to coronary artery disease and heart failure.
For access to the full length article, please
sign in.
